
Know your Dizziness
Correct diagnosis is half the cure.
To make the correct diagnosis the clinician will need dizziness specific information from the patients.
The aim of the "Know Your Dizziness-KnowledgeBase" section is to provide some basic information on dizziness and vertigo to equip the patients/family for their consultation with the clinician.
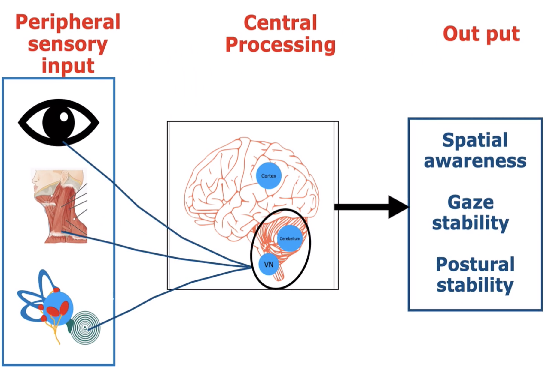
How do we achieve balance control?
Balance control is a complex mechanism achieved by interactions between peripheral (sensory) and central (brain) structures.
Peripherally, vision, proprioception and vestibular (Inner ear) systems contribute to balance control. Centrally, structures within the brainstem, cerebellum and several other brain areas are involved in processing the balance signals.
The multi-sensory balance signals help achieve balance control out puts such as spatial orientation, gaze stability and postural stability. The vestibular system is exclusively responsible for sensing static position and dynamic movements of the head.
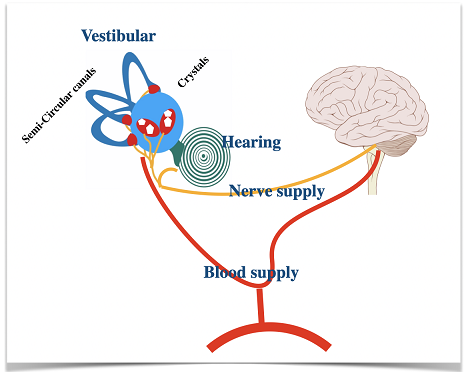
What is the role of Vestibular System in balance control?
The vestibular system is located within the labyrinth/ inner ear along with the hearing apparatus. The vestibular system has a vestibule and 3 semicircular canals. Both the vestibule and semicircular canals have movement sensing jelly-like structures; however, Otoconia, the calcium carbonate crystals are present only within the vestibule, making the vestibule sensitive to gravity. Endolymph circulates within the vestibular system.
The vestibular nerve carries head position/ movement-related signals from the SCC and vestibule to the brainstem and cerebellum. The vestibular system receives its blood supply from the arteries that supply the above brain structures.
Do you know what dizziness & vertigo actually means?
Dizziness is a non-specific term used to describe a range of sensations. It can mean a range of different descriptions. However, the clinicians will categorise the descriptions into one of the following subtypes.
- Vertigo- Room-spinning or head-spinning sensation
- Pre-syncope- Faint-like feeling
- Disequilibrium - Unsteadiness
- Light-headedness
While some descriptions are meaningful and easy to comprehend others can be confusing and difficult to describe. Do not worry/ do not spend too much time describing the type of dizziness. To diagnose the underlying condition cause(s) of dizziness other characteristics are more helpful than the type of dizziness. Please pay more attention to the following
- Triggers (what brings the dizziness on),
- Duration (how long the dizziness last)
- Frequency (how often the dizziness occur) and
- Accompanying symptoms (hearing loss, sensitivity to bright lights & headache etc.)

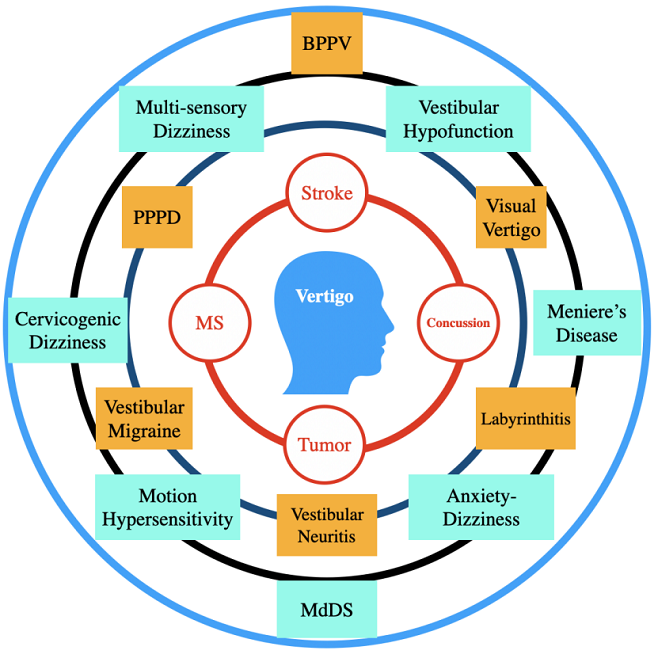
What causes dizziness/vertigo?
Mal de débarquement syndrome (MdDS)
MdDS sufferers experience sensations of rocking, bobbing or swaying. These symptoms are more pronounced when standing still compared to walking.
MdDS occurs commonly after a cruise, however, sometimes MdDS like symptoms can occur without being on a cruise (Pseudo MdDS).
Readaptation of the VRT and sensory reweighing training helps reduce the MdDS symptoms. In cases of the pseudo MdDS, diagnosing and addressing the underlying cause of it, in addition to the readptation of the VOR and sensory reweighing training will help improve the symptoms.
Dizziness/vertigo is not a condition it is merely a symptom of an underlying condition. The causes of dizziness/vertigo can range from trivial causes such as feeling dizzy when we stand up quickly after sitting for a while to life-threatening conditions such as stroke and brain tumour. Fortunately, the most commonly occurring dizziness are due to benign conditions such as BPPV, Vestibular migraine, age-related multi-sensory balance issues and PPPD.
The vestibular-specific examination is helpful to diagnose most of the common vestibular disorders. Except in rare cases such as stroke and brain tumours, investigations such as MRI, CT scan and blood tests are not helpful to diagnose dizziness.
What is Vestibular Rehabilitation (VRT)?
Vestibular rehabilitation (VRT) is a specialised form of therapy intended to alleviate both the primary and secondary problems due to vestibular disorders. It is an exercise-based program primarily designed to reduce vertigo and dizziness, reduce gaze instability, and/or reduce imbalance and fall risk as well as address any secondary impairments that are a consequence of the vestibular disorder (VeDA)
How vestibular disorders are treated?
When it comes to the treatment of vestibular disorders “One-Size-Fits-All” will not work as each conditions will require specific treatments. Treatment needs to be customised and patient-centred.
Below are some condition-specific treatments :
- BPPV- Posterior canal- Canalithiasis- Epley manoeuvre
- BPPV- Posterior canal- Cupulolithiasis- Semont liberatory manoeuvre
- BPPV- Lateral canal- 360° BBQ roll
- BPPV- Anterior canal - Deep Head Hanging Manoeuvre
- Vestibular Hypofunction - VOR Adaptation
- Bilateral Vestibular Hypofunction - Slow VOR, COR Substitution
- PPPD- Customised VRT
- Poor sensory integration - Customised balance exercises
- Vestibular migraine - Customised VRT, Food & lifestyle modification
- Risk of falls- Customised balance exercises

VESTIBULAR FACTS!
- 1 in 3 people aged 40 years and 85% of people aged 80 years and above are suffering from vestibular balance problems ( Y Agrawal ).
- Over 80% of people with vestibular disorders are reported to be experiencing impacts in their daily activities and seek medical help or sick leave ( Neuhauser HK)
- Causes of Dizziness
- Vestibular causes
- Non-Vestibular causes
- Multi-sensory issues
- Bronstein AM,et al found that due to dizziness
- 27% people change their job
- 21% gave up work
- 50% reduced efficiency at work
- 57% disruption in social life,
- 35% family difficulties
- 50% difficulties with travel
- A UK based study found that patients had to wait nearly two years (on average 90+ weeks, range - 14 to 202 weeks) for the diagnosis and treatment of their BPPV. (D. W. Fife, John Fitzgerald 2005)
- Delayed diagnosis and treatment of BPPV will have negative impacts on both patients and their carers in terms of cost and quality of life Vestibular patients are not optimally managed in the Emergency Department. BPPV patients are unnecessarily tested with CT and MRI and treated with vestibular medications, which are not indicated (David E. Newman-Toker)
- Frequent error occurs in the acute setting in differentiating central from peripheral causes of vertigo. Over 40% of initial ED diagnoses were later corrected; 6% of serious cases were revised as benign and 23% serious cases were revised as benign.
- Peripheral vestibular diagnostic tests (Dix-Hallpike, Head Thrust Test etc.)for dizziness are scarcely used in the primary care
Medication therapy for dizziness
- Medical therapy for BPPV: Routine use of vestibular suppressants are not recommended for the treatment of BPPV
- Use of vestibular suppressants in patients with BPPV could obscure the clinical presentation of BPPV such as positional nystagmus during BPPV.
Harmful effect of vestibular medication
Long term use of vestibular medication can potentially ….
- Interfere with central compensation for a vestibular disorder
- Cause cognitive dysfunction
- Increase the risk of falls
- Drug-induced Parkinsonism
Vestibular Physiotherapy for dizziness
- Vestibular physiotherapy is effective to correctly diagnose and safely treat all types of BPPV
- Vestibular physiotherapy is safe and effective to treat vestibular hypofunction (labyrinthitis, vestibular neuritis etc.)
- Vestibular physiotherapy reduces dizziness, improves balance, reduces the risk of falling and improves balance confidence and activities of daily living.
References
- Agrawal Y, Carey JP, et al. Disorders of balance and vestibular function in US adults: data from the National Health and Nutrition Examination Survey, 2001–2004. Arch Intern Med. 2009; 169(10): 938–944.
- Neuhauser HK. Epidemiology of vertigo. Curr Opin Neurol. 2007; 20(1):40–46.
- Bronstein AM, Golding JF, et al. The social impact of dizziness in London and Siena. J Neurol. 2010; 257(2):183–190
Bronstein AM, Golding JF, et al. The social impact of dizziness in London and Siena. J Neurol. 2010; 257(2):183–190
- Fife D, Fitz Gerald JE: Do patients with benign paroxysmal positional vertigo receive prompt treatment? Analysis of waiting times and human and financial costs associated with current practice. Int J Audol 2005;44:50–7.
- Newman-Toker DE, Camargo CA, Hsieh Y, et al. Disconnect between charted vestibular diagnoses and emergency department management decisions: a cross-sectional analysis from a nationally representative sample. Acad Emerg Med. 2009;16:970-977.
- Royl G, et al. Dizziness in the emergency room: diagnoses and misdiagnoses. Eur Neurol 2011;66:256–63.
- Dros J, Maarsingh OR, van der Horst HE, Bindels PJ, ter Riet G, et al. (2010) Tests used to diagnose dizziness in primary care: a systematic review. CMAJ 182(13): E621–631.
- https://vestibular.org/article/what-is-vestibular/causes-of-dizziness/.
- https://www.parkinsons.org.uk/sites/default/files/2018-09/FS38%20Drug%20induced%20parkinsonism_0.pdf
- Hillier, S. L., & Hollohan, V. (2007). Vestibular rehabilitation for unilateral peripheral vestibular dysfunction (Cochrane Review). In The Cochrane Collaboration (Issue 4). Chichester, England: Wiley.
- Bhattacharyya N, Gubbels SP, Schwartz SR, et al. Clinical practice guideline: benign paroxysmal positional vertigo (update). Otolaryngol Head Neck Surg. 2017 Mar;156(3 suppl):S1-S47.


DizzyCare Clinic
Oaktree House, Oaktree Rise,
Codsall, Wolverhampton
WV8 1DP



